Treatment of an Infected Femoral Nonunion Using the Ilizarov Method
1. Medical History and Background (Patient with Multiple Previous Surgeries)
The patient presented with a complex case of infected femoral nonunion, following several failed initial surgical procedures:

Initial treatment: Internal fixation using a plate and screws.

Outcome: Removal of the plate due to hardware failure and infection of the surgical site.
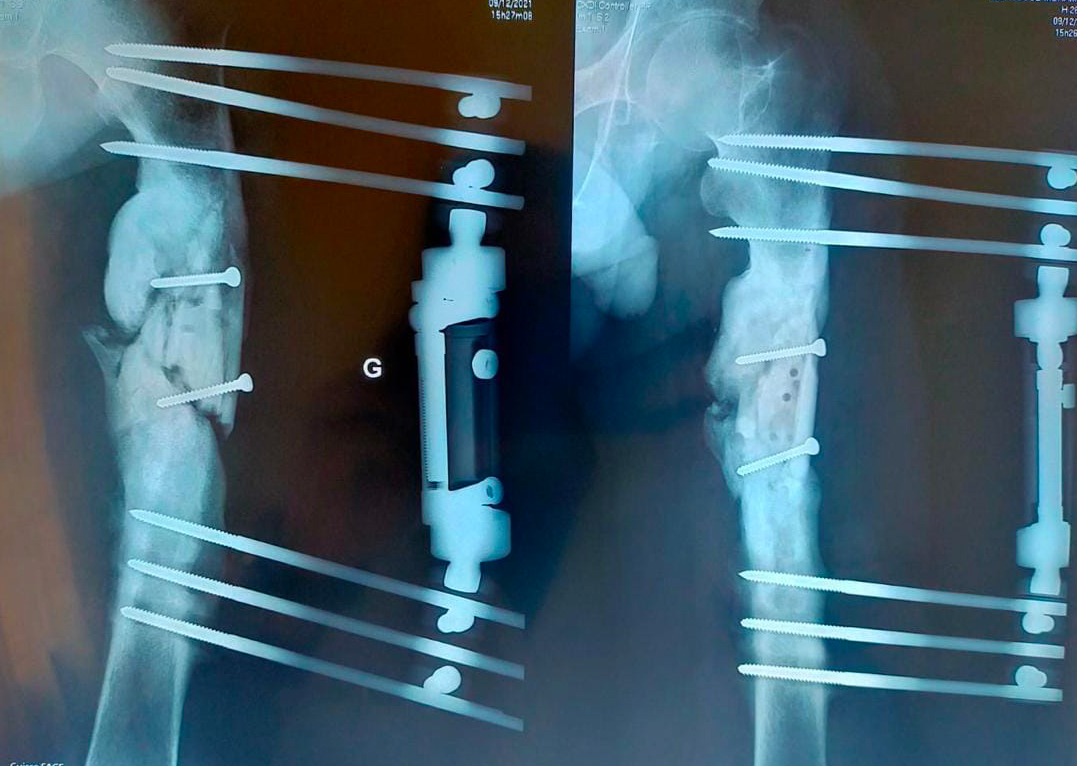
Second-stage treatment: Application of a linear external fixator associated with a minimal temporary treatment (Monster).
2. Surgical Management and Therapeutic Strategy
Due to persistent infection, the presence of bone sequestra, and a major bone defect, the patient was managed according to a multi-stage strategy based on the Ilizarov method:
Stage 1: Debridement and Limb Shortening
- Extensive fistulectomy and sequestrectomy (removal of all necrotic and infected bone tissue).
- Significant femoral shortening of approximately 12 cm to bridge the bone defect, bring healthy bone ends into contact, and achieve infection control.
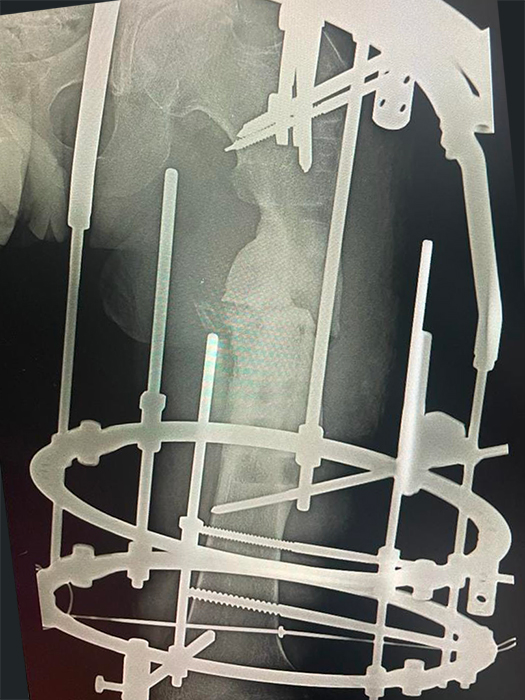
- Application of a circular Ilizarov external fixator.

Stage 2: Reconstruction Using the Ilizarov Method
- Performance of a distal femoral osteotomy to initiate distraction osteogenesis (gradual bone lengthening).
3. Clinical and Radiological Outcome
The postoperative course was particularly favorable, allowing all therapeutic objectives to be achieved:
- Infection control: Complete eradication of the infectious focus through the initial debridement.
- Bone union: Successfully achieved at the site of the femoral nonunion.
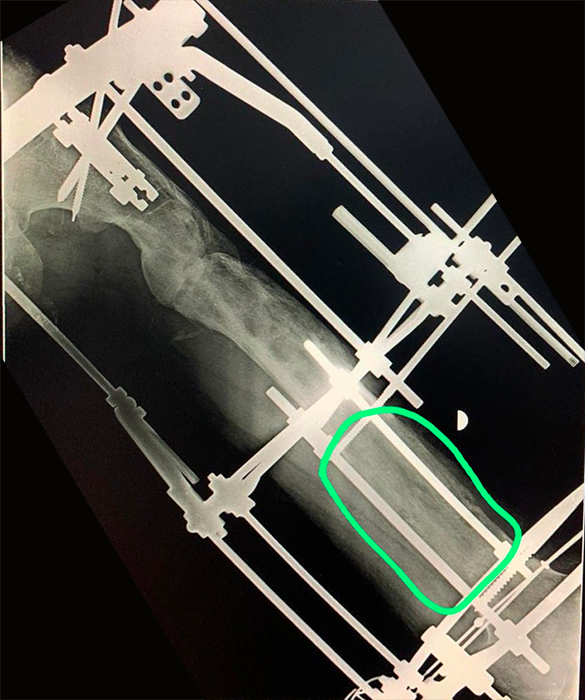
- Bone regeneration: Progressive lengthening at the distal osteotomy site functioned perfectly.
- Limb length restoration: The patient fully recovered the original length of the lower limb (compensating for the 12 cm shortening).
Conclusion
At follow-up, treatment using the Ilizarov method successfully salvaged the limb of this patient who had undergone multiple previous surgeries. An excellent functional recovery was observed, with full weight-bearing ambulation and definitive bone healing. The infection is considered cured.

Final radiograph showing fracture union and regeneration of 12 centimeters of bone