Reconstruction of a major 8-cm tibial bone defect using bone transport according to the Ilizarov method after failure of multiple previous surgical procedures, including treatment with a circular external fixator.

Clinical view showing leg shortening and deformity
The management of segmental tibial bone defects represents a major challenge in orthopedic and trauma surgery. We report the case of a patient presenting with a massive 8-cm bone defect at the junction of the proximal and middle thirds of the tibia, following an open fracture and multiple previous surgical failures. While previous attempts using circular external fixators had failed, the implementation of a reconstruction strategy based on segmental bone transport after distal osteotomy achieved complete defect filling and final bone union without the need for additional bone grafting. After a 14-month follow-up period, the external fixator was removed, providing the patient with full functional recovery, painless ambulation, and a significant improvement in quality of life.

Tibial bone defect
1. Introduction and Case Presentation
This patient had a significant history of lower-limb trauma following an open fracture of the leg. Initially managed at other institutions, he underwent an extensive and repetitive treatment course, totaling ten (10) surgical procedures over a period of seven and a half years. Among these procedures, treatment with a circular Ilizarov external fixator had been attempted but failed, leading to its premature removal due to the absence of progressive bone healing. Upon admission to our department, the initial clinical and radiological assessment revealed the following:
Infectious status: No clinical or laboratory signs of active infection (clean surgical site).
Bone status: Presence of a critical segmental bone defect measuring 8 cm, located precisely at the junction between the proximal and middle thirds of the tibia.
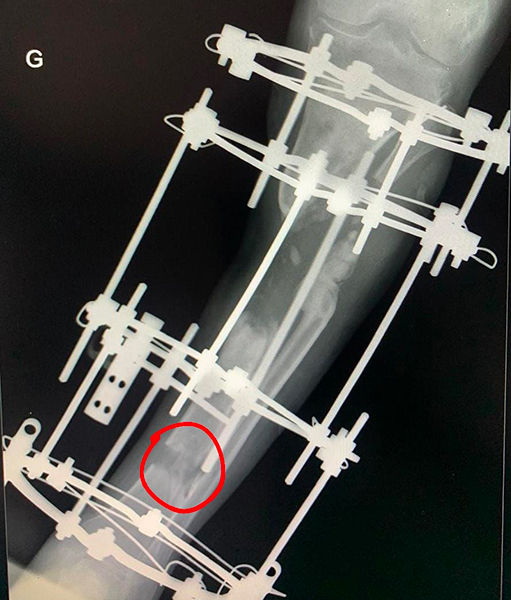
Distal tibial osteotomy with initiation of bone transport
2. Therapeutic Strategy and Surgical Technique
Given a bone defect of this magnitude (8 cm), immediate shortening techniques and conventional massive bone grafting procedures were ruled out in order to preserve limb length and avoid donor-site morbidity. The chosen treatment strategy relied on the principles of mechanotransduction and guided bone regeneration through segmental bone transport. The surgical protocol consisted of several key phases:
Phase 1: Corticotomy and Distraction
A distal tibial corticotomy was performed within a healthy metaphyseal region.
A new rigid external fixation system was applied.
Transport of the intermediate bone segment from the distal to the proximal region was initiated at a standardized rate in order to induce the formation of new regenerate bone within the distraction gap.
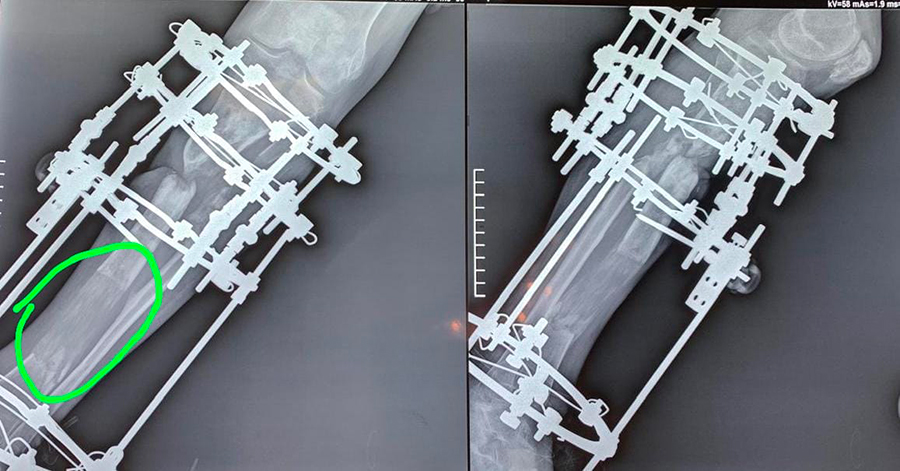
Early consolidation of the regenerate bone and contact between the transported fragment and the proximal metaphysis
Phase 2: Docking Phase and Release of Fibrous Adhesions
Bone transport was continued until direct contact was achieved between the fixed proximal fragment and the mobile intermediate fragment (docking site). As commonly occurs during prolonged tissue transport procedures, dense fibrous adhesions developed at the docking site, preventing optimal bone impaction. A targeted surgical procedure was therefore performed to excise these adhesions and release the docking site.
Phase 3: Compression and Consolidation (Without Bone Grafting)
Once the docking site had been released, an axial compression phase was initiated through the external fixator. In accordance with the principles of Ilizarov distraction osteogenesis, no autologous or allogeneic bone graft was used.
3. Results and Clinical Outcome
The total duration of treatment with the external fixator was 14 months, encompassing the transport, release, compression, and regenerate maturation phases. The anatomical and functional outcomes were excellent:
Bone defect reconstruction: Complete restoration of the 8-cm defect through regenerated bone formation.
Bone union: Full cortical union was achieved both at the distraction site (distal metaphyseal regenerate) and at the proximal docking site under compression.
Current functional status: The external fixator was successfully removed. The patient demonstrates stable, smooth, full weight-bearing ambulation without pain. Clinical benefit and patient satisfaction are excellent.

Final radiograph demonstrating complete bone union
4. Discussion and Conclusion
This case demonstrates the remarkable effectiveness of bone transport for the management of critical tibial bone defects, even after multiple surgical failures spanning nearly a decade. Unlike the two previous cases in which limb shortening was favored, bone transport made it possible to: Treat a critical-sized defect (8 cm) beyond the capabilities of simple bone grafting.
Maintain equal lower-limb length without creating limb-length discrepancy.
Avoid the morbidity associated with iliac crest harvesting or vascularized fibular transfer procedures.
Meticulous management of the docking site, particularly through surgical release of naturally occurring fibrous adhesions, remains a crucial step in achieving stable biological fusion and durable bone continuity. In conclusion, bone transport remains the gold-standard limb-salvage technique for functional amputations secondary to segmental bone loss of the leg.
