Clubfoot (Talipes Equinovarus - CTEV) is a common congenital deformity. However, when left untreated or neglected during childhood, it progresses into a so-called neglected form in adulthood. In these patients, the medial and posterior musculotendinous, capsular, and ligamentous structures undergo severe contracture, associated with significant osseous architectural alterations.
The management of these rigid deformities represents a major surgical challenge. The Ilizarov method (progressive distraction using a circular external fixator) has become a preferred alternative to extensive corrective arthrodesis or excessive bone resections, allowing preservation of limb length while minimizing soft tissue complications.
Clinical Presentation and Initial Assessment
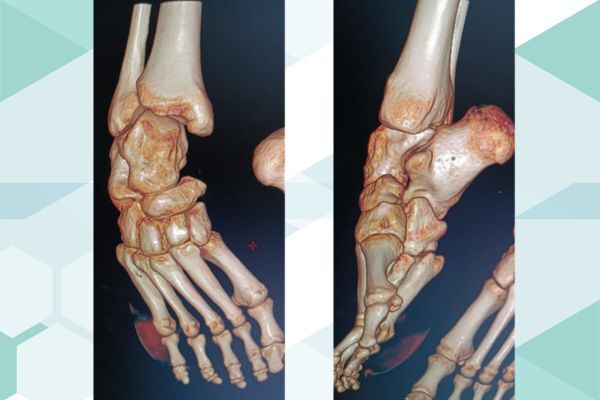
The initial clinical examination reveals a rigid three-dimensional foot deformity, characteristic of neglected clubfoot:
Severe fixed equinus: An irreducible plantar flexion that limits or prevents normal plantigrade heel contact with the ground.
Adduction and Varus: Medial deviation of the forefoot (adduction) associated with inversion of the calcaneopedal block (varus).
Skin changes: Areas of hyperkeratosis or callosities along the lateral border of the foot, reflecting chronic abnormal weight-bearing during walking.
Treatment Strategy: The Ilizarov Method
Given the rigidity of the soft tissues and the severity of the deformity, acute one-stage surgical correction carries a significant risk of skin necrosis and neurovascular complications. Therefore, a gradual correction using an Ilizarov external fixator was chosen.
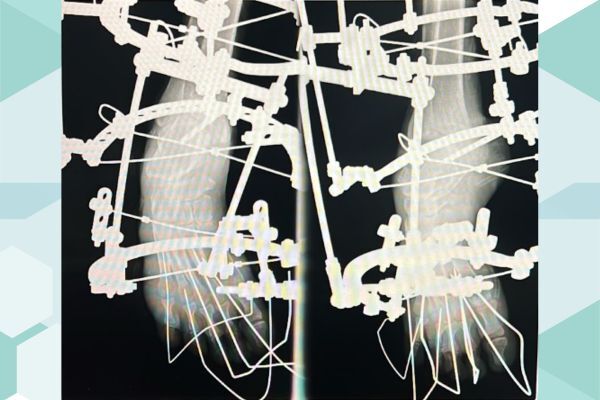
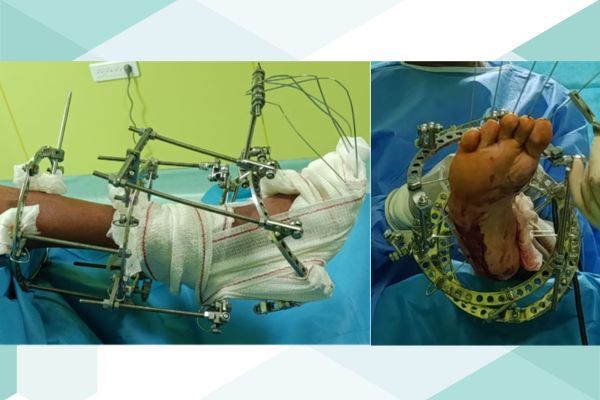
1. External Fixator Assembly
The surgical construct (as seen on the postoperative radiographs) includes:
Proximal rings: Attached to the tibial segment (diaphysis/metaphysis) using Schanz pins and/or transfixing Kirschner wires, providing a stable foundation.
A calcaneal half-ring or stirrup: Connected to the heel bone to control and reduce the equinus deformity while correcting the varus component.
Forefoot fixation: Allowing the application of opposing distraction forces to correct adduction and restore the overall anatomical alignment of the foot.
Threaded adjustment rods: Connecting the various segments to enable precise daily micrometric distraction.
2. Correction Protocol (Distraction)
After a postoperative latency period of several days, progressive correction is initiated by either the patient or the medical team:
Rate: Fractionated millimetric distraction (typically 1 mm per day divided into four adjustments) to allow gradual biological lengthening of the contracted soft tissues (distraction histogenesis).
Objectives: To progressively bring the foot to a right angle (90° relative to the leg) and align the forefoot with the hindfoot.
Postoperative Clinical Outcomes
Strict application of Ilizarov principles allows the achievement of:
Complete correction of equinus: The foot regains a neutral position or slight dorsiflexion, facilitating full plantigrade heel support.
Correction of adduction: The forefoot is realigned, restoring the overall anatomical shape of the foot.
Preservation of soft tissues: Progressive stretching avoids excessive tension on the skin, thereby eliminating the risk of wound dehiscence or local skin necrosis.
Conclusion
The treatment of neglected adult clubfoot using the Ilizarov external fixator remains a highly specialized yet remarkably effective technique. By avoiding extensive bone-sacrificing procedures and respecting the often fragile soft tissue envelope, it enables the achievement of a plantigrade, stable, painless, and functional foot, dramatically improving both functional outcomes and the patient's quality of life.